

Rối Loạn Lưỡng Cực Là Gì: Triệu Chứng, Giai Đoạn Hưng Cảm Và Trầm Cảm, Cách Nhận Biết Sớm
If you searched for “rối loạn lưỡng cực là gì: triệu chứng, giai đoạn hưng cảm và trầm cảm, cách nhận biết sớm”, you’re probably trying to put words to something that feels confusing—or intense. Let’s make it clear, human, and practical (without turning it into a medical textbook). 🧠

What is bipolar disorder (rối loạn lưỡng cực) — in plain English?
Bipolar disorder is a mental health condition where your mood, energy, activity level, and thinking can shift in episodes—most notably:
- Manic or hypomanic episodes (hưng cảm / hưng cảm nhẹ): elevated or irritable mood with increased energy and behavior changes
- Depressive episodes (trầm cảm): low mood and loss of energy/motivation with cognitive and physical symptoms
The key idea: these aren’t ordinary mood swings. They’re episodes that are intense enough (and long enough) to disrupt how you function at work, school, in relationships, sleep, money decisions, and safety.
The takeaway is clear: Bipolar disorder isn’t “being emotional.” It’s a pattern of episodic mood states that can seriously impact your life—especially when it isn’t recognized early.
Bipolar disorder types (and why the labels matter)

Clinicians typically talk about several presentations. You don’t need to memorize them, but you do need to know what they imply:
| Type | Core pattern | What often stands out |
|---|---|---|
| Bipolar I | At least one manic episode (may include depression) | Mania can be severe, sometimes includes psychosis or hospitalization risk |
| Bipolar II | Hypomania + major depression | Depression can be the dominant problem; hypomania can be missed or even “liked” |
| Cyclothymic disorder | Chronic ups/downs that don’t meet full episode criteria | Long-term instability that still affects relationships, self-image, and work |
| Other specified / unspecified | Bipolar-like symptoms that don’t fit cleanly | Real impairment can still be present even without a neat label |
Let’s be honest: many people only seek help during depression—because hypomania can feel like productivity, confidence, or finally “being yourself.” That’s one reason bipolar disorder is often misidentified as unipolar depression.
For a broader emotional perspective (less clinical, more “felt experience”), you can also read Rối Loạn Lưỡng Cực: Hiểu Để Thương, Thương Để Hiểu.
The manic phase (giai đoạn hưng cảm): symptoms you shouldn’t ignore 🔥

Mania is more than “high energy.” It’s a distinct shift where your brain is essentially pressing the gas pedal—hard.
Common manic symptoms (hưng cảm)
You might notice:
- Decreased need for sleep (not insomnia—more like “I slept 3 hours and I’m amazing”)
- Inflated self-esteem or grandiosity (“I’ve figured it all out,” “I’m unstoppable”)
- Racing thoughts, rapid speech, jumping topics
- Increased goal-directed activity (work, social life, projects) or agitation
- Impulsivity / risky behavior:spending sprees 💳reckless drivingimpulsive sexsubstance usequitting a job suddenly
- Irritability (many people expect euphoria—irritability is just as common)
- In severe cases: psychosis (delusions, hallucinations)
Hypomania vs mania (quick clarity)
Hypomania is like a “lighter” version, but it still matters—especially because it can precede depression.
| Feature | Hypomania (hưng cảm nhẹ) | Mania (hưng cảm) |
|---|---|---|
| Intensity | Noticeable change, often still functioning | Severe disruption in functioning |
| Duration (typical diagnostic minimum) | ~4 days | ~7 days (or any duration if hospitalization is needed) |
| Psychosis | No | Can occur |
| Risk level | Can still lead to harm | Higher risk; safety can become urgent |
If your “up” state is causing damaged relationships, unsafe decisions, or you’re not sleeping but feel wired—don’t romanticize it as “finally productive.” That’s a trap.
The depressive phase (giai đoạn trầm cảm): what it looks like in bipolar disorder 🌧️

Bipolar depression can look like major depression—but there are patterns that sometimes hint it’s part of bipolarity.
Common depressive symptoms
- Persistent low mood, emptiness, or hopelessness
- Loss of interest/pleasure (anhedonia)
- Low energy, heavy body feeling
- Sleep changes (too much or too little)
- Appetite/weight changes
- Concentration problems, slowed thinking
- Guilt, worthlessness
- Thoughts of death or suicide
Why bipolar depression is often missed
Because many people:
- seek help only when depressed
- don’t recognize hypomania as a symptom
- are told they have “stress” or “burnout”
- may be treated as unipolar depression first
If you want to compare depression vs stress vs something deeper, this internal guide is useful: Stress hay trầm cảm? Cách phân biệt để chăm sóc bản thân đúng cách.
Mixed features: when “up” and “down” happen at the same time ⚡🌧️

Not everyone experiences clean, separate episodes. Some people have mixed features, like:
- depressed mood + racing thoughts
- agitation + hopelessness
- insomnia + low mood
- high energy + suicidal thinking
This can be one of the most dangerous presentations because the energy to act can increase while mood remains painfully low.
Early signs: how to recognize bipolar disorder sooner (cách nhận biết sớm) 👀
Early recognition isn’t about self-diagnosing—it’s about noticing patterns that deserve a proper evaluation.
1) Your sleep changes predict your mood
A classic early signal is sleep reduction without fatigue, followed by behavior shifts:
- talking faster
- planning big projects
- spending more
- feeling unusually confident or irritable
2) People close to you notice “a different you”
Sometimes you don’t feel “sick”—you feel activated. But others might say:
- “You’re not listening.”
- “You’re talking over everyone.”
- “You’re intense.”
- “You’re making scary decisions.”
3) Episodes have a “before and after”
Bipolar patterns tend to be episodic: you can often identify:
- a ramp-up phase
- a peak (manic/hypomanic or depressive)
- a crash or recovery period
4) Depression keeps returning—or responds oddly to antidepressants
Some people report:
- antidepressants triggering agitation, insomnia, or “wired” energy
- repeated depressive episodes with brief periods of unusually high drive in between
Quick “pattern check” table
| Clue | Why it matters |
|---|---|
| Repeated cycles of “superhuman productivity” then crash | Suggests episodic mood shifts, not just motivation issues |
| Decreased sleep with high energy | Classic signal of (hypo)mania |
| Impulsive money/relationship decisions during “up” states | Behavioral marker that often shows up early |
| Family history of bipolar disorder | Increases likelihood—worth mentioning to a clinician |
| Mixed symptoms (agitated depression) | Often missed but clinically important |
Bipolar vs “normal mood swings,” ADHD, and borderline personality — a fast comparison
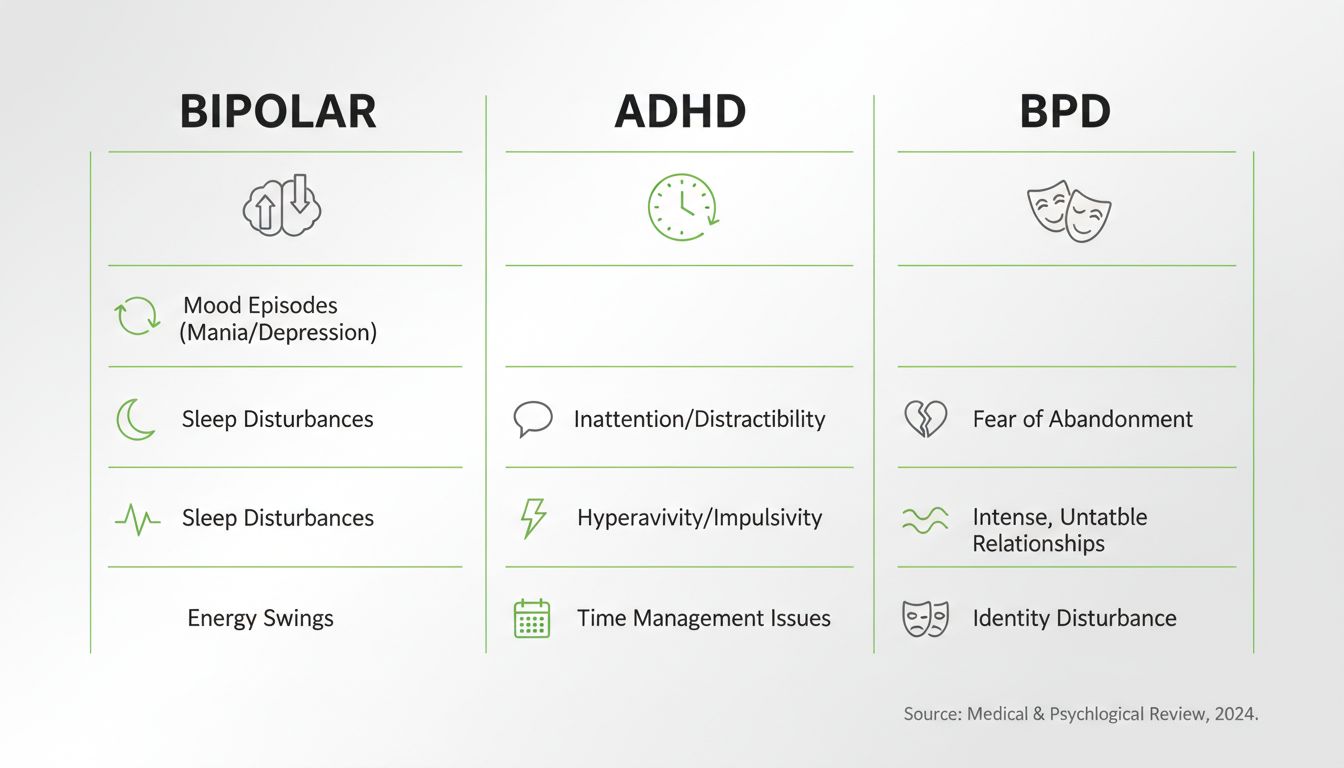
Because confusion is common, here’s a clean breakdown:
| Feature | Bipolar disorder | ADHD | Borderline personality disorder (BPD) | |---|---|---| | Pattern | Episodic mood states | More chronic attention/impulsivity | Mood shifts often triggered by relationship stress | | Sleep | Reduced need during (hypo)mania | Can have insomnia, but not classic reduced-need pattern | Sleep disruption often tied to emotional distress | | Core issue | Mood episode physiology | Executive function regulation | Emotion regulation + fear of abandonment patterns | | Duration | Days to weeks (or longer) | Lifelong pattern | Rapid shifts (hours to days), strongly situational | | Risk behaviors | Often during mania | Impulsivity baseline | Impulsivity tied to emotional triggers |
Reality check: overlap happens. You can have more than one condition. The point is to guide a proper assessment.
Why early support matters (without fear-mongering)

Untreated bipolar disorder can increase risk for:
- relationship breakdowns
- job/academic instability
- financial damage from impulsive decisions
- substance misuse
- self-harm or suicide risk (especially during mixed or depressive states)
But the upside is real: with correct diagnosis and consistent care, many people achieve stable, meaningful lives.
A short video that helps you understand bipolar disorder better 🎥
When to seek professional help (and what to say)

You should consider reaching out if:
- you suspect hypomania/mania (especially decreased need for sleep + risky choices)
- depression is recurring, severe, or includes suicidal thoughts
- people around you are worried about your behavior changes
- your life feels like it’s being driven by cycles you can’t control
What to tell a professional (so you don’t get brushed off)
Bring specifics:
- sleep changes (hours/night)
- spending/impulsive decisions
- speech speed, racing thoughts
- timeline of episodes (even rough)
- family history
- any antidepressant reactions
If you’re exploring different ways to get support, this comparison helps you choose what fits: Therapy online vs therapy trực tiếp: nên chọn hình thức hỗ trợ tâm lý nào?.
And if you want a safe place to start with a human who gets it, you can check out Đồng Hành Cùng Tiên (Ngọc Tĩnh - Hỗ Trợ Tâm Lý).
Safety: if you’re in danger right now

If you have thoughts of harming yourself or you feel unable to stay safe, treat it as urgent:
- In the US, you can call or text 988 (Suicide & Crisis Lifeline).
- If you’re in immediate danger, call 911 or go to the nearest ER.
You don’t have to “prove” you’re unwell enough. If it feels unsafe, it’s unsafe.
Key takeaways you can remember today ✅
- Bipolar disorder is defined by episodes of (hypo)mania and/or depression—not everyday moodiness.
- Mania/hypomania often shows up first as less sleep + more energy + more risk.
- Bipolar depression can look like typical depression, so the “up” episodes are critical to mention.
- Early recognition is about spotting patterns over time, not labeling yourself in one bad week.
- Getting the right support earlier can prevent the “silent damage” (money, relationships, safety) that episodes can cause.
If you want to keep learning in a gentle, stigma-free way, you can browse more articles at Khám phá thêm từ blog Ngọc Tĩnh.